David K. Guilkey, Lisa M. Calhoun, Ilene S. Speizer
Few investigators examine program diffusion because they lack data from outside the intervention areas. Using data collected from state-level surveys, David Guilkey, Lisa Calhoun and Ilene Speizer demonstrate the spread of a Nigerian family planning program to non-target rural and urban areas through the diffusion processes of mass communication, social influence, and social learning.
Innovations can spread through direct exposure to an intervention or indirectly through other pathways such as mass media. Messages may thus be shared and discussed outside a specific intervention area or through social influence and social learning (Montgomery and Casterline, 1996; Kohler et al., 2001). This spread of interventions beyond their original target area is often discussed in terms of diffusion of programs or innovations (Dearing, 2009). Diffusion is rarely studied because of a lack of data available for areas outside of the program target areas. In a recently published paper (Guilkey et al., 2020), we examine diffusion of the Nigerian Urban Reproductive Health Initiative (NURHI) to areas outside the target cities.
NURHI was funded by the Bill & Melinda Gates Foundation to increase modern contraceptive use in six major urban areas of Nigeria using intervention activities designed to change demand for family planning (mass media and social mobilization), improve service delivery (training of providers and provision of a full range of methods), and attract additional funding and stakeholder support for family planning programming (Krenn et al., 2014). At the time of NURHI launch, it was hoped that activities in the major urban areas would diffuse or spread beyond the target areas, but no specific plan was undertaken to measure this diffusion.
This study provides a unique opportunity to measure the influence of indirect pathways – such as diffusion of ideas or information through, for example, interactions at the interpersonal level or through mass communication – on modern contraceptive use. This study uses representative data from two Nigerian states (Kaduna and Oyo) that surround two NURHI program cities (Kaduna and Ibadan) to study diffusion of program activities to rural areas and other urban areas in each target state.
This study explores how three separate aspects of diffusion influence modern contraceptive use in non-target cities. Mass communication, an impersonal channel through which ideas may diffuse, was explored by asking respondents from non-target cities about exposure to program campaign activities. Social influence, which makes certain behaviors normative, was explored through a proxy question which asked whether respondents thought that they would receive praise from other community members for using modern contraception. Finally, social learning, whereby individuals learn through interacting with other people about their experiences, was explored by looking at the effect of lagged community-level modern contraceptive use on modern contraceptive use in the next period, similar to what was done in earlier analyses (Montgomery and Casterline, 1993; Rosero-Bixby and Casterline, 1994).
We estimated cross-sectional models for analyses exploring the relationship between exposure to mass communication variables and our proxy for social influence on modern contraceptive use. We used a pseudo-longitudinal panel dataset constructed from reproductive calendar data to explore lagged individual and community-level contraceptive use (a commonly used proxy for social learning) on modern contraceptive use.
Mass communication
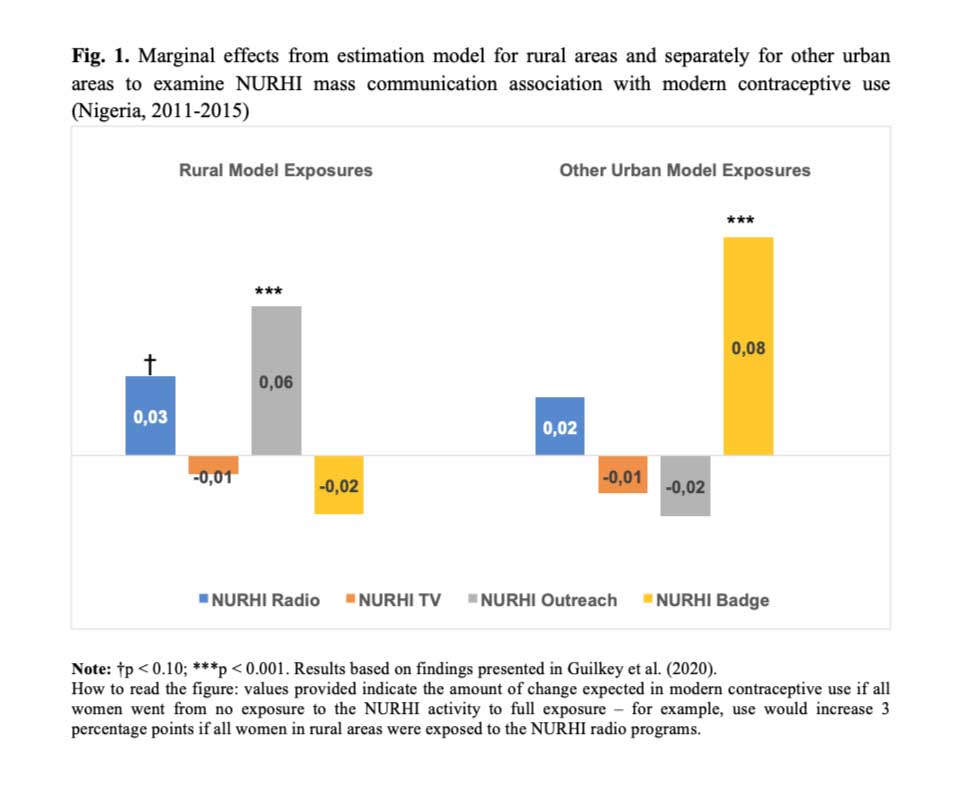
The NURHI program, implemented in 6 cities in Nigeria from 2011-2015, focused on changing norms, ideational factors and behavior through implementation of a diverse set of demand-side program activities (Krenn et al., 2014) aiming to increase modern contraceptive use in the six cities. Modern contraception includes female sterilization, implants, intrauterine devices (IUD), injectables, oral contraceptive pills, emergency contraception, male or female condoms, and lactational amenorrhea (LAM). We measured the association of women’s use of modern contraception with exposure to four components of the NURHI program in cross-sectional models with socioeconomic control variables that included age, education, wealth, and religion among other factors. The four program components were exposure to NURHI family planning messages on the radio, exposure to NURHI-supported programs or advertisements on television, having seen the NURHI badge worn by a service provider, and exposure to NURHI-initiated outreach events that included an outreach worker talking about family planning at life events (e.g., weddings, naming ceremonies, graduations, freedom ceremonies, and Christmas/Eid).
Figure 1 shows the estimated average marginal effects for these models separately for rural areas and other urban areas, that is, the increase in the proportion of women who would use modern contraception if they went from no exposure to a program component to exposure.
In the model for rural areas, exposure to NURHI radio programming and NURHI outreach were positive and significant while only exposure to the NURHI badge had a significant positive effect in other urban areas. Thus, there appears to be evidence of diffusion through the mass communication diffusion channel, although for only a few aspects of the NURHI program.
Social influence
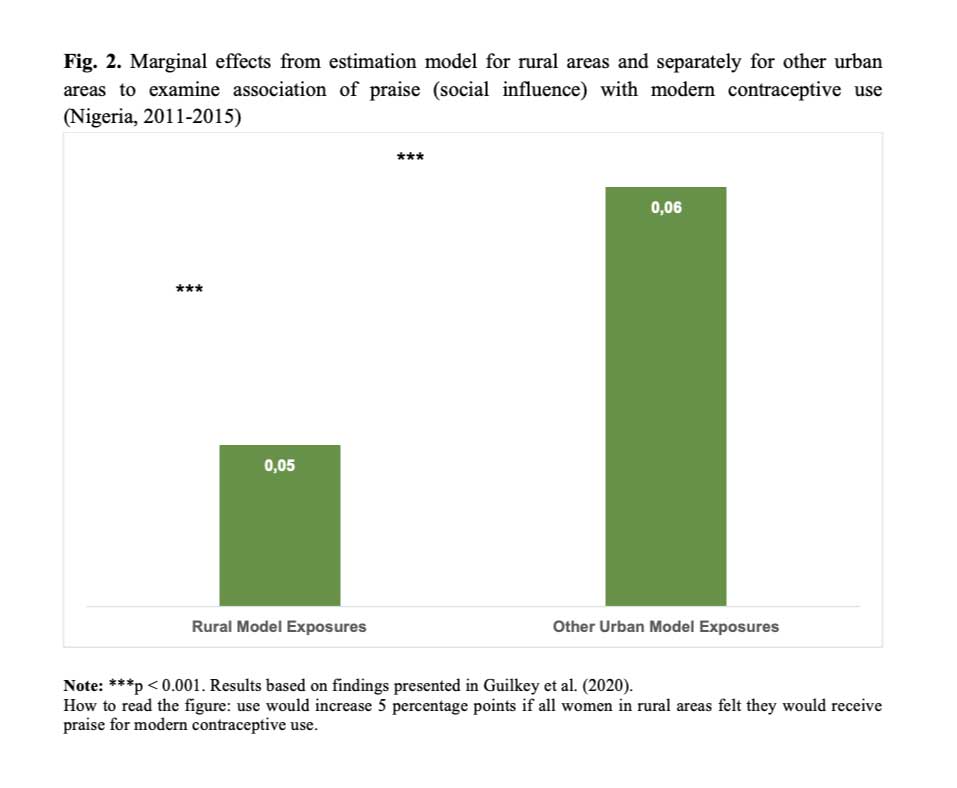
A key focus of the NURHI program was to change attitudes and perceptions around the use of modern contraception with the hope that this would result in increased modern contraceptive use. We estimated models that include our proxy measure of social influence: whether the woman thought that she would receive praise from community members for using modern contraception. Presented in Figure 2 are the estimated average marginal effects for the model that includes praise as the key social influence variable. As seen in the figure, the praise variable is strongly significant for both rural and other urban areas and the impact is quite large – the marginal effects indicate a 5-6 percentage point increase in modern contraceptive use when the respondent feels that she would receive praise for modern use versus feeling that she would not. These results provide clear evidence that this measure of social influence has a positive association with modern contraceptive use in rural areas and non-target program cities.
Social learning
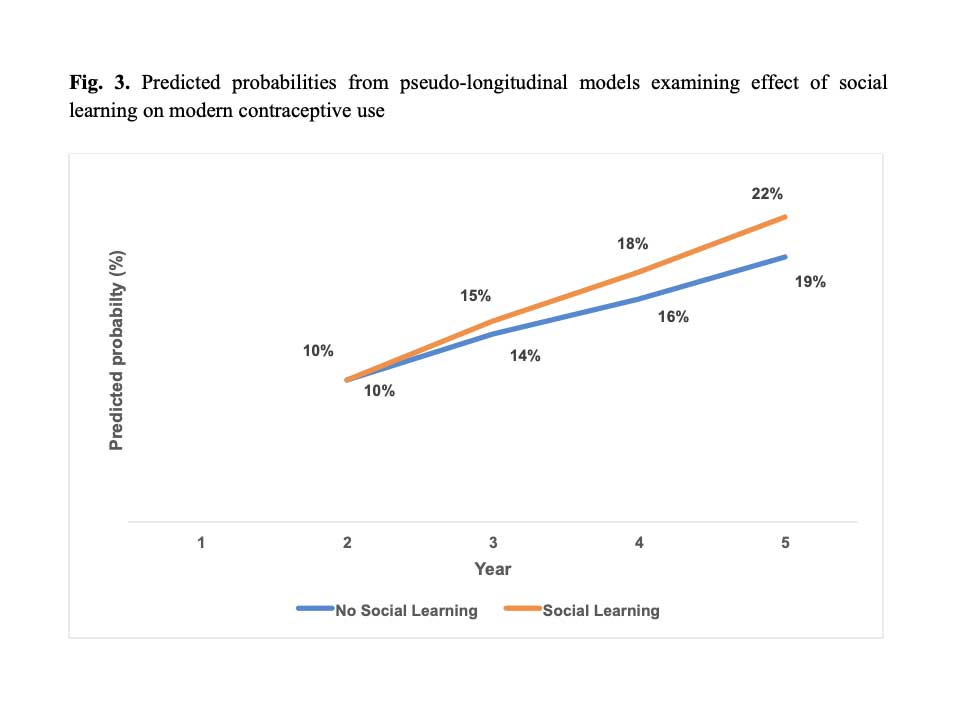
We examined lagged community modern contraceptive use to determine if this proxy for social learning influences modern contraceptive use in Kaduna and Oyo states in addition to the effect of the respondent’s own previous use of contraception. After estimating the model, we used a dynamic simulation approach to predict the percentage of women using modern contraception each year over the five-year period, assuming that no women are using modern contraception in year 1 in this simulation. We present the predicted probabilities of modern contraceptive use under two scenarios: social learning and no social learning (Figure 3). Under the social learning scenario, there is evidence of social multiplier effects whereby lagged community use of contraception is larger in each subsequent year and stimulates higher probabilities of modern contraceptive use in the years that follow.
The findings from this study have important implications for donors and program implementers. The results suggest that programmatic gains made during program implementation may continue to have effects, and even be built upon, after the end of implementation and this should be measured and considered from the outset.
References
- Dearing, J.W. (2009). Applying Diffusion of Innovation Theory to intervention development. Research on Social Work Practice, 19(5), 503-518. doi:10.1177/1049731509335569.
- Guilkey, D.K., Escamilla, V., Calhoun, L.M., & Speizer, I.S. (2020). The examination of diffusion effects on modern contraceptive use in Nigeria. Demography, 57(3), 873-898. doi:10.1007/s13524-020-00884-6.
- Kohler, H.P., Behrman, J.R., & Watkins, S.C. (2001). The density of social networks and fertility decisions: Evidence from South Nyanza District, Kenya. Demography, 38, 43–58.
- Krenn, S., Cobb, L., Babalola, S., Odeku, M., & Kusemiju, B. (2014). Using behavior change communication to lead a comprehensive family planning program: the Nigerian Urban Reproductive Health Initiative. Global Health Science and Practice, 2(4), 427-443. doi:10.9745/GHSP-D-14-00009.
- Montgomery, M.R., & Casterline, J.B. (1993). The diffusion of fertility control in Taiwan: Evidence from pooled cross-section time-series models. Population Studies, 47, 457–479.
- Montgomery, M.R., & Casterline, J.B. (1996). Social learning, social influence, and new models of fertility. Population and Development Review, 22, 151–175.
- Rosero-Bixby, L., & Casterline, J. B. (1994). Interaction diffusion and fertility transition in Costa Rica. Social Forces, 73, 435–462.
No comments:
Post a Comment