Equity Considerations for Digital Technologies for Family Planning During COVID-19 and Beyond
The race to adapt to COVID-19 has resulted in a shift to virtual formats for health care training and service provision. This has amplified reliance on digital technologies. What does this mean for women seeking services but lacking the knowledge of and access to these technologies?
The Digital Gender Gap
We know a digital gender gap impacts women’s access and ability to use digital technologies, including smartphones, social media, and the internet. This problem also exacerbates existing inequities, including poverty, education, and geographic access. The digital gender gap is worse for women who have lower levels of education, low income, are older, or are living in rural areas. Across low- and middle-income countries, those in sub-Saharan Africa and South Asia face the most significant challenges connecting to digital technology. In South Asia, there is 65% mobile phone ownership, with a 23% gender gap in ownership, leaving up to 203 million women unable to access a mobile phone and associated digital services (see the figure below). In addition to gaps in mobile phone ownership, there is also a gap in mobile internet usage. For example, in Bangladesh, there is a 52% gender gap in mobile internet use. This usage gap is 29% in Nigeria and 48% in Uganda (GSMA Mobile Gender Gap Report, 2020).
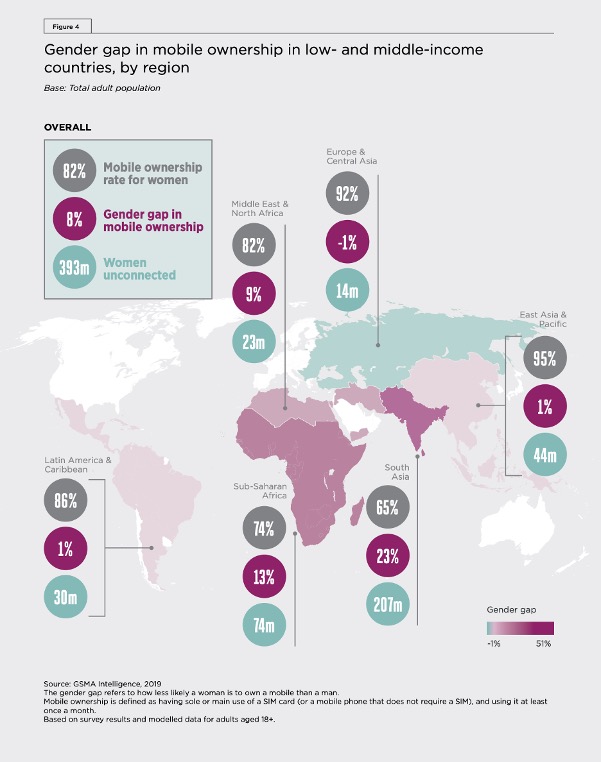
Figure source: Page 15 of GSMA Mobile Gender Gap Report (2020). Click for an accessible version.
A variety of potential factors including social norms and affordability, among others, contribute to the digital gender gap. For generations, social norms have designated men as responsible for technological aspects of daily life, relegating many women to non-technological household roles. Social norms that influence whether a woman receives higher education or can maintain employment outside the home also impact digital technology use.
In general, social media may not be the most welcoming space for women due to unchecked harassment in online spaces where gender norms and violence are perpetuated. In India, 58% of women report experiences of online harassment, and 40% reduced their device use or deleted accounts as a result as shared in this Gender & Digital Webinar. A presenter at this webinar, Kerry Scott, associate faculty at Johns Hopkins School of Public Health (JHSPH), reminds us that the cost of maintaining a phone line can be prohibitive. In some cases, women may regularly change their mobile numbers to get cheaper rates, which can lead to disconnection from relevant services and resources.

Relatively lower phone ownership, internet access, and social media presence mean women already have limited options to access and share information as it relates to their health. The problem is only compounded when this barrier intersects with other factors, including:
- Income.
- Geography.
- Education levels.
The digital gender gap further enforces inequity in knowledge management for global health. Digital platforms themselves reflect gender biases: Men are the primary stakeholders in their development and design. Women are not necessarily intended to be the target user. This, when combined with the obstacles to accessing these platforms, can have a snowball effect that perpetuates the gap. The digital gender gap extends across many fields and populations, posing a serious challenge to program designers and implementers.
The Digital Gender Gap and COVID-19: What Does This Mean for Access to Family Planning Information and Services?
While many family planning programs had already adopted digital technology to support some service delivery tasks, such as counseling, follow-up, and referral, this shift accelerated during the COVID-19 pandemic. Are decision-makers considering the gaps in access to and use of digital technologies as this shift continues? The mHealth researchers and practitioners we spoke with warned that programs, policies, and general COVID-19 adaptations can do more to address the digital gender gap. For example, a common adaptation is phone-based hotlines to discuss family planning options with a counselor, but are those hotlines accessible by rural women? By women who don’t have much training on how to use a mobile phone? By women whose husbands control their phone use? These are important questions for us to think about when implementing a digital adaptation.
Digital health innovations will best serve clients and support providers only if steps are taken to ensure equity in implementation. Recognizing how your family planning program can integrate gender-equitable concepts and strategies will help lessen the exclusionary effects of the digital gender gap.
Program Spotlight: Digital Literacy to Dismantle Gender Inequality
The Strong Enough Girls Empowerment Initiative (SEGEI) partners with a non-governmental organization in Nigeria on the “Girl Advocates for Gender Equality” project. Together, they are training 36 adolescent girls across Nigeria to participate in bi-weekly WhatsApp mentorship sessions on topics including:
- Sexual- and gender-based violence.
- Girls’ education, financial literacy.
- Women in leadership.
- Science, technology, engineering, and math (STEM).
The girls use their phones to capture pictures and videos of outreach to other girls outside of the program, creating a cascade of learning in their communities. See some of their posts on Instagram.
Digital Health Amidst a Digital Gender Gap: How to Adapt Effectively
Here are some other short- and long-term changes your program can make to integrate gender considerations with mHealth. (Francesca Alvarez, IGWG; Onyinye Edeh, SSGEI; Erin Portillo, Breakthrough ACTION; and Kerry Scott, JHSPH, contributed to these tips.)
Short-Term Changes to Make/Considerations
Long-Term Changes to Make/Considerations
So, has the digital gender gap become even more exclusionary? We would argue that it has. The digital gender gap itself may not have expanded (many women may have more access to digital technologies today than they did five years ago), but the nature of the gap has evolved so that the impact of not having access creates greater disadvantages than before. Now, not having a phone or knowing how to use it could mean that a woman has fewer opportunities to gain information about family planning services in her area, while those who can fully participate in digital spaces can better address their reproductive health needs and goals.
The experts we spoke with reminded us that mHealth is not a “silver bullet.” Digital health, if implemented alongside larger health systems strengthening programs, can be transformative. But the full benefit of this transformation will only come if the digital gender gap is accounted for and steps are taken to mitigate its impact on women’s access to and use of digital health technologies. It should be part of a solution, capitalizing on existing relationships and strengths, not an isolated innovation.
No comments:
Post a Comment